Introduction to Physiology
The Science of How the Body Works

What Is Physiology?
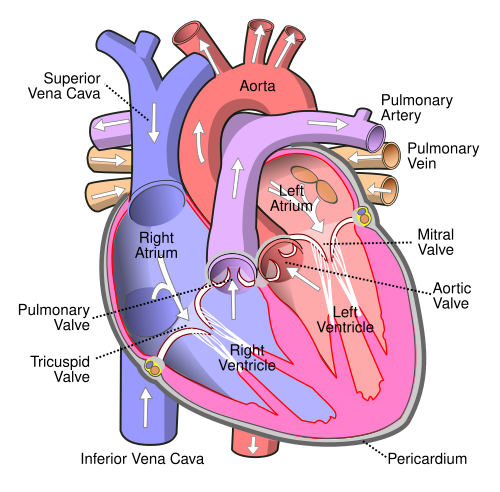
Physiology is the branch of biology and medicine that studies the normal functions of living organisms and their parts. Derived from the Greek physis (nature) and logos (study), physiology asks: How does the heart pump? How do neurons fire? How does the kidney filter blood? It is the foundational science bridging anatomy (structure) with clinical medicine (dysfunction and disease). Physiology is inherently dynamic Ś it studies processes, not just parts.
Homeostasis: The Central Principle
The most fundamental concept in physiology is homeostasis Ś the ability of the body to maintain a stable internal environment despite external changes. Claude Bernard (1813¢1878) coined the idea of the milieu intķrieur (internal environment). Walter Cannon later named it homeostasis. Key variables maintained include body temperature (37░C ▒ 0.5░C), blood pH (7.35¢7.45), blood glucose (70¢110 mg/dL), plasma osmolarity (280¢295 mOsm/L), and blood pressure (~120/80 mmHg). Disruption of homeostasis is the definition of disease.
Feedback Control Systems
Homeostasis is maintained through feedback loops. Negative feedback loops oppose a change and restore the setpoint Ś for example, when body temperature rises, sweating and vasodilation cool the body. This is the most common type. Positive feedback amplifies a change Ś for example, during childbirth, oxytocin causes uterine contractions that press the baby against the cervix, which triggers more oxytocin Ś a self-amplifying cycle that ends only with birth. Blood clotting and the action potential in neurons are also positive feedback events.
Cell as the Unit of Physiology
All physiological functions ultimately reduce to cellular processes. The cell membrane (phospholipid bilayer with embedded proteins) controls what enters and leaves. Ion channels, pumps (Na?/K?-ATPase), and carriers maintain electrochemical gradients essential for nerve impulses, muscle contraction, and nutrient absorption. Mitochondria produce ATP via oxidative phosphorylation Ś the energy currency for every active physiological process. Understanding cell physiology is the key to understanding organ physiology.
Levels of Physiological Study
Physiology operates across multiple scales: molecular physiology (protein conformational changes, enzyme kinetics, gene expression), cellular physiology (action potentials, receptor signaling, secretion), organ physiology (cardiac output, lung mechanics, glomerular filtration), systems physiology (cardiovascular regulation, hormonal axes), and whole-organism physiology (exercise response, stress adaptation, aging). Modern physiology integrates all these levels through computational modeling and systems biology approaches.